As UA inhibits mTOR, is it better to cycle it? How often? Is it better to take it in the morning? In the evening? With or without food? 
In terms of half-life, I found this:
(to compare: “The half-life of rapamycin is 58–63 hours (~ 3 days).”)
In this mice study they use 2.5 mg/kg UA (that’s 10x less than in the 2023 Buck Institute paper that showed life extension) + 25 mg/kg green tea extract EGCG. The UA+EGCG combination seems about 15% more potent than UA alone looking at figures and tables (guesstimate). Interestingly, they still cycled UA even with this low dose: “3 times per week for 4 months.” And they still had good results.
If my above reasoning is correct (maintenance dose of 90 Mitopure pills per year), then with EGCG, you can instead use only 77 pills. You can probably even decrease to 60 pills/y, meaning one Mitopure Softgels sachet ($125 to which you need to add the cost of EGCG). Of course, we don’t have evidence yet evidence this dosing regimen in human adults would have any benefits.
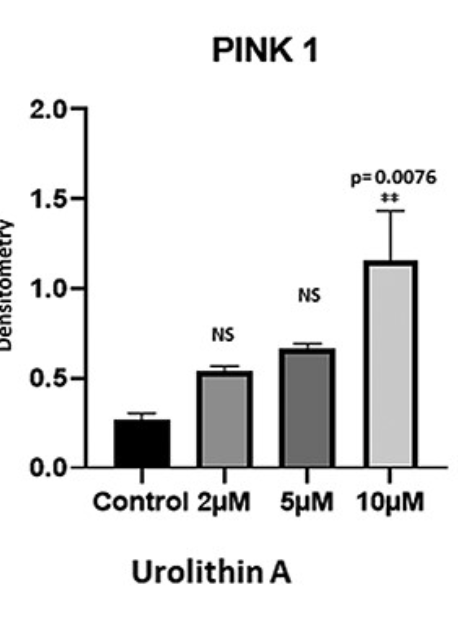
I don’t know how to make sense of the 10x difference in terms of dose between the two studies. The authors of the 2022 paper (that used the lowest 2.5 mg/kg dose) wrote: “We recently optimized doses of mitophagy enhancers urolithin A, actinonin, tomatidine and nicotinamide riboside in HT22 cells” and they cite this paper: Protective effects of mitophagy enhancers against amyloid beta-induced mitochondrial and synaptic toxicities in Alzheimer disease 2021. They only tested 0, 2, 5, and 10 μM of UA directly on cells, and there was a quasi-linear dose-response relationship. Would 100 μM be even better?
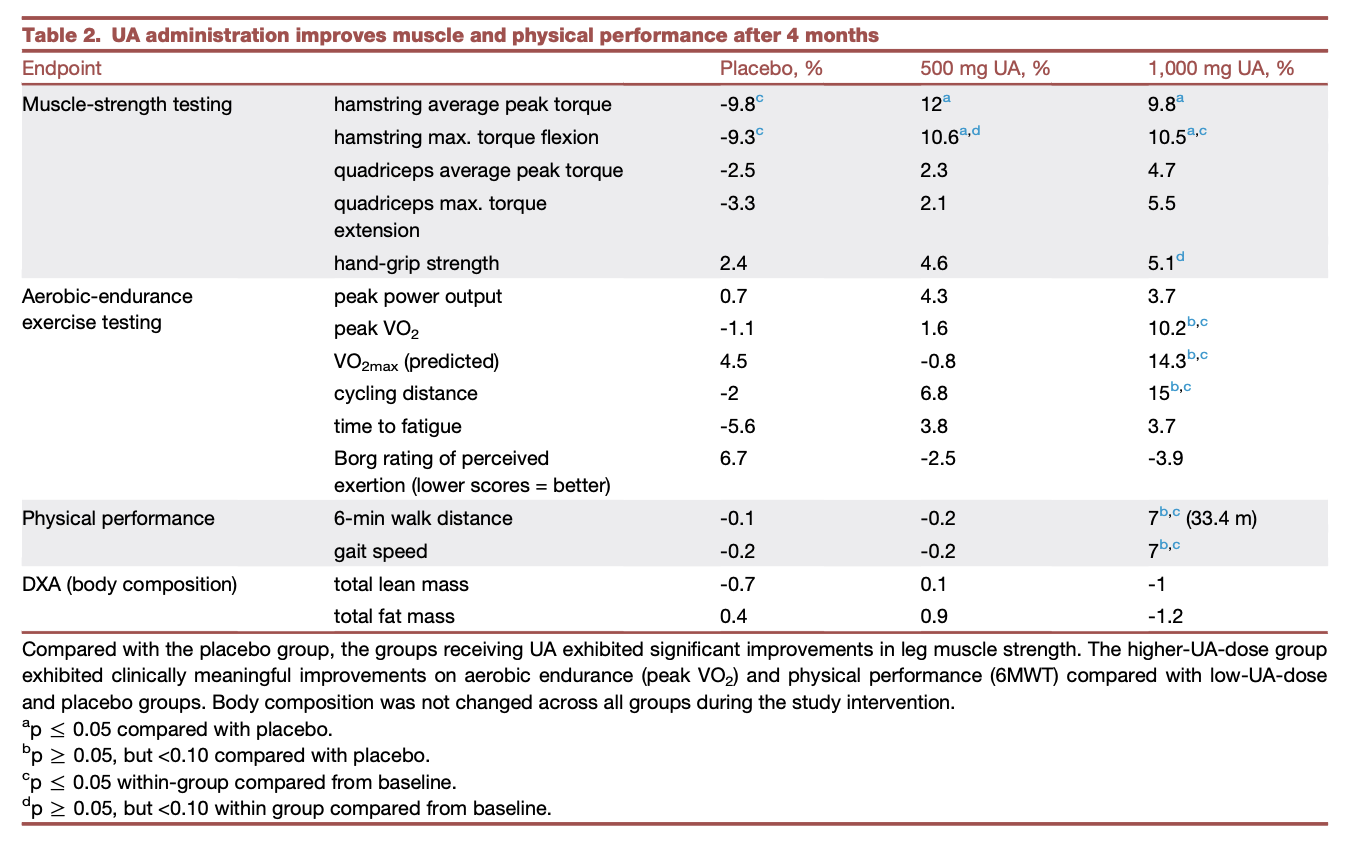
In the Mitopure study on middle-aged humans, they compared 500 mg (the commercial Mitopure dose) to 1,000 mg, and found that 1,000 mg was better.
In this 2023 study (by Amazentis) they even “supplemented with UA oral targeting 50mg/kg/day” on mice (Study 2)! Urolithin A induces cardioprotection and enhanced mitochondrial quality during natural aging and heart failure (preprint)
Anyway, I bought one Mitopure pack (60 pills). I’ll see what I do. I’m hesitating between (with or without EGCG in each case, TBD):
- Following the recommended Mitopure regimen (500 mg/d = 2 pills) for a month then see or,
- 1 pill (250 mg) every other day, one week on, one week off,
- 2 pills (500 mg) per week.
Feedback welcome 
Also, Solgar UK answered my email regarding Mitopure:
Unfortunately we don’t sell this product here in the UK. It sells well abroad but there isn’t enough demand for it in this country at the moment.
A lot of our products are available to buy from reputable online retailers such as Amazon, or from specialist import/export retailers.
If other UK residents email them we could maybe convince them that there’s enough demand. poke @Walter_Brown